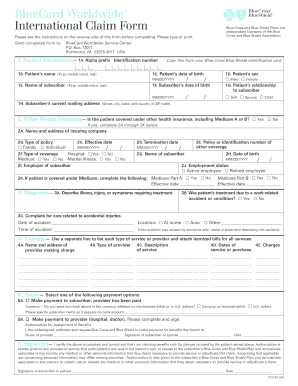
Otherwise the Default Option will be used. BlueCard Worldwide International Claim Form.
 Submitting Your Claims Alberta Blue Cross
Submitting Your Claims Alberta Blue Cross
Check with the Provider to be sure no claim has been submitted.

Blue shield reimbursement form. Blue Cross Blue Shield Settlement co JND Legal Administration PO Box 91390 Seattle WA 98111. Employees who are part of PPO plans that have the Blue Shield Rx Program can use this direct reimbursement form when they have used. If you select the Alternative Option you must submit relevant data or records showing a higher contribution percentage.
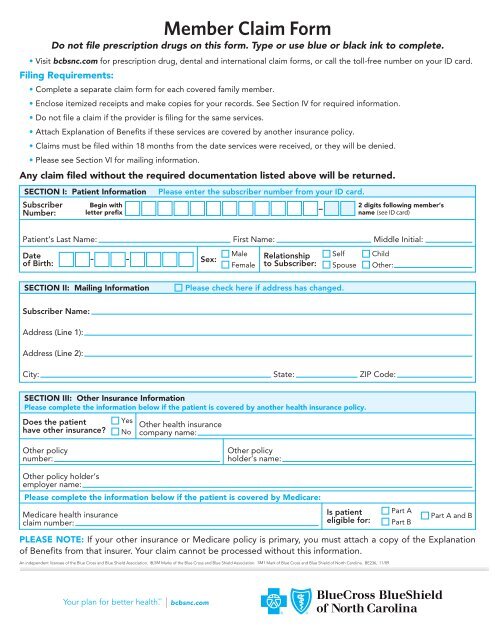
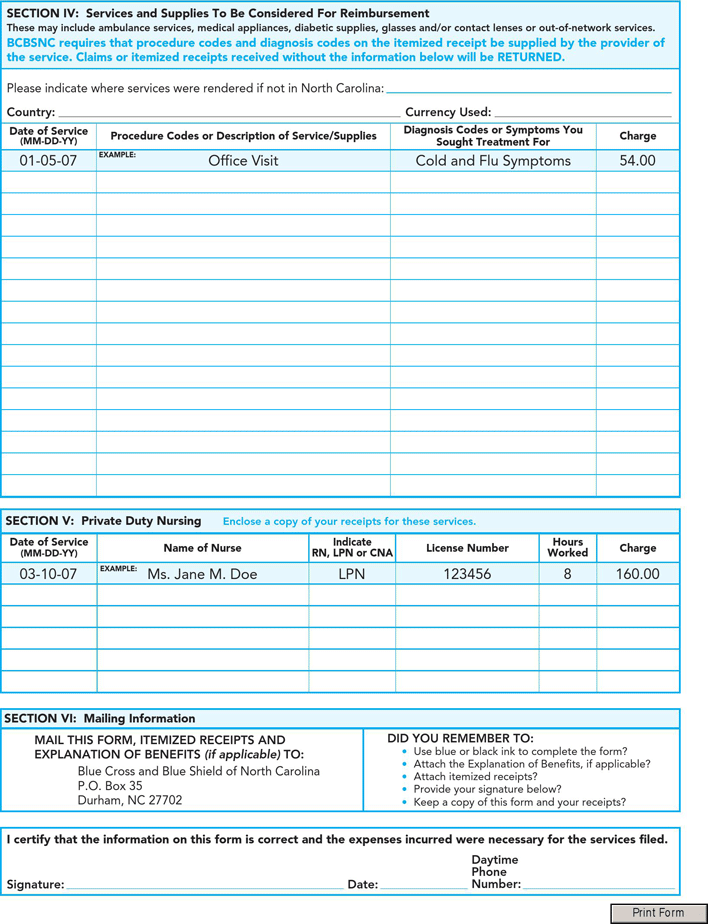
Box 35 Durham NC 27702. You can use these claim forms to ask us for reimbursement. The Blue Cross and Blue Shield name and symbols are registered marks of the Blue Cross.
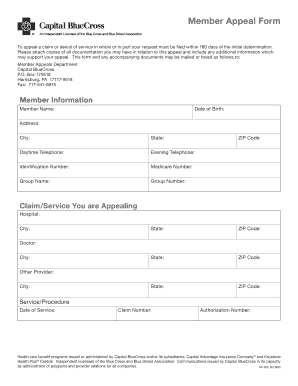
Complete a separate Subscriber Claim Form for each patient and for each provider. Accept the terms and conditions. RELATIONSHIP TO SUBSCRIBER Self Spouse Dependent If the patients last name is different from the subscribers please attach a statement explaining the relationship H.
SUBSCRIBERS CURRENT MAILING ADDRESS Street City State and Country or ZIP Code 2. Refer to the COVID-19 Preparedness page for temporary information related to servicing members in response to COVID-19. Renewal Audit Package You and your dependents must live in Massachusetts to renew your individual health plan with Blue Cross Blue Shield of MA.
Follow the steps below to access the claim form. Attach a copy of the itemized bill. Claim Forms Claim Forms.
Get And Sign Blue Cross Blue Shield Overseas Medical Claim Form. Box 805107 Chicago Illinois 60680-4112 A Division of Health Care Service Corporation a Mutual Legal Reserve Company an Independent Licensee of the Blue Cross and Blue Shield Association 2289341015 Claim Form. Blue Cross Blue Shield of Rhode Island is an independent licensee of the Blue Cross and Blue Shield Association.
Duplicate claims will not only be rejected but may delay payment of the original claim. Submitting Form Information MAIL THIS FORM ITEMIZED RECEIPTS AND EXPLANATION OF BENEFITS if applicable TO. A form authorizing Blue Cross Blue Shield of Massachusetts to send specific information to a specific individual.
Use this form to show your eligibility. Click on Claim Forms and choose the form preferred For more information and to confirm your coverage please call Customer Service. You will be going to a new website operated on behalf of the Blue Cross and Blue Shield Service Benefit Plan by a third party.
Complete only those sections of this form. Instructions Please complete one Member Medical Claim Form per health care provider. Subscribers Statement of Claim This form is to be used ONLY when the Provider of Service does not submit your claim directly to Blue Shield.
Download PDF PDF 110KB Blue Shield of California Prescription Drug Benefit - Direct Reimbursement Claim. The providers name and address and Federal tax ID or National Provider Identifier NPI the diagnosis or the symptoms of illness. Blue Cross and Blue Shield of North Carolina Senior Health DBA Blue Cross and Blue Shield of North Carolina is an HMO D-SNP plan with a Medicare contract and a contract with the North Carolina Medicaid program.
If you are requesting payment for multiple providers you must submit a separate claim form for each provider. Communications may be issued by Horizon Blue Cross Blue Shield of New Jersey in its capacity as administrator of programs and provider relations for all its companies. Enter the 3 character prefix from the members ID.
Reimbursement DMR form or contact customer service. If you were on a cruise youll use the same claim form for reimbursement of medical. Blue Cross Blue Shield of Massachusetts will make a reimbursement decision within 30 calendar days of receiving a completed request form.
Blue Cross Blue Shield of Massachusetts will make a reimbursement decision within 30 calendar days of receiving a completed request form. Reimbursement is sent to the members address on file with Blue Cross. Employees use this form if the out-of-country provider directly billed Blue Shield of California for covered services.
Blue Cross and Blue Shield of North Carolina. Reimbursement is sent to the members address on file with Blue Cross. The bill should show.
HOW TO SUBMIT YOUR CLAIM. If you use a provider outside of the network you will need to complete and file a claim form for reimbursement. Instructions for submitting your claim are on the claim form available here.
The protection of. Section 4 Examples of qualified wellness activities and caregiver services Section 5 Submit your form. Important instructions Use a separate form A.
Blue Cross and Blue Shield of North Carolina Blue Cross NC is an independent licensee of the Blue Cross and Blue Shield Association. When required sufficient documentation shall include an attestation. Blue Cross and Blue Shield of Illinois PO.
Enroll Elect Apply Forms Enroll Elect Apply Forms. Wellness Caregiver reimbursement form. The following resources provide you with the information needed to administer Blue Cross and Blue Shield of Texas BCBSTX.
Overseas members should use the Overseas Medical Claim Form. Just choose the form based on your group or plan and the service. Member Reimbursement Donor Egg and Sperm Complete and submit this form to request reimbursement.
Sometimes the form is called Member Application for Payment Consideration which is the same as a claim form. Reimbursement may be considered taxable income so consult your tax advisor. Youll go to a page that explains the form and has a link to download it.
BLUE CROSS BLUE SHIELD CLAIM FORM You may be eligible to receive a cash payment if you are an Individual Insured Group and their employees or Self-Funded Account and their employees that purchased or were enrolled in a Blue Cross or Blue Shield BCBS health insurance or. If your other insurance or Medicare policy is primary you must attach a copy of the Explanation of Benefits from.
 Download Blue Cross Blue Shield International Medical Claim Form For Free Formtemplate
Download Blue Cross Blue Shield International Medical Claim Form For Free Formtemplate
 Https Www Ohio Edu Sites Default Files Sites Hr Files Medical Claim Form Pdf
Https Www Ohio Edu Sites Default Files Sites Hr Files Medical Claim Form Pdf
 Blue Cross Blue Shield International Fillable Claim Form Fill Online Printable Fillable Blank Pdffiller
Blue Cross Blue Shield International Fillable Claim Form Fill Online Printable Fillable Blank Pdffiller
 Member Claim Form Blue Cross And Blue Shield Of North Carolina
Member Claim Form Blue Cross And Blue Shield Of North Carolina
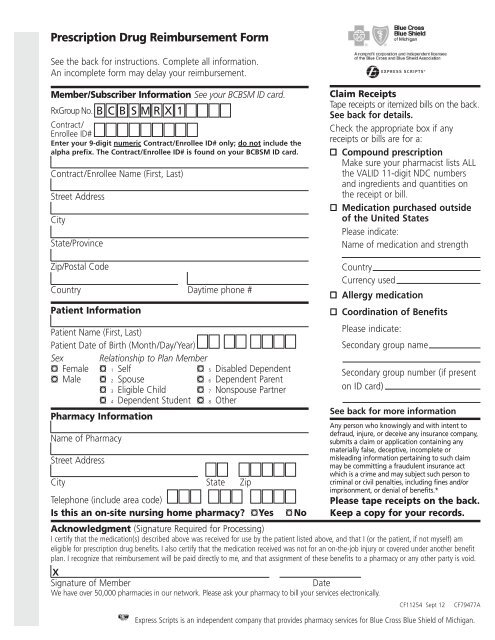 Rx Group Number Bcbsmrx1 Reimbursement Form Blue Cross
Rx Group Number Bcbsmrx1 Reimbursement Form Blue Cross
 Reimbursement Claim Fill Online Printable Fillable Blank Pdffiller
Reimbursement Claim Fill Online Printable Fillable Blank Pdffiller
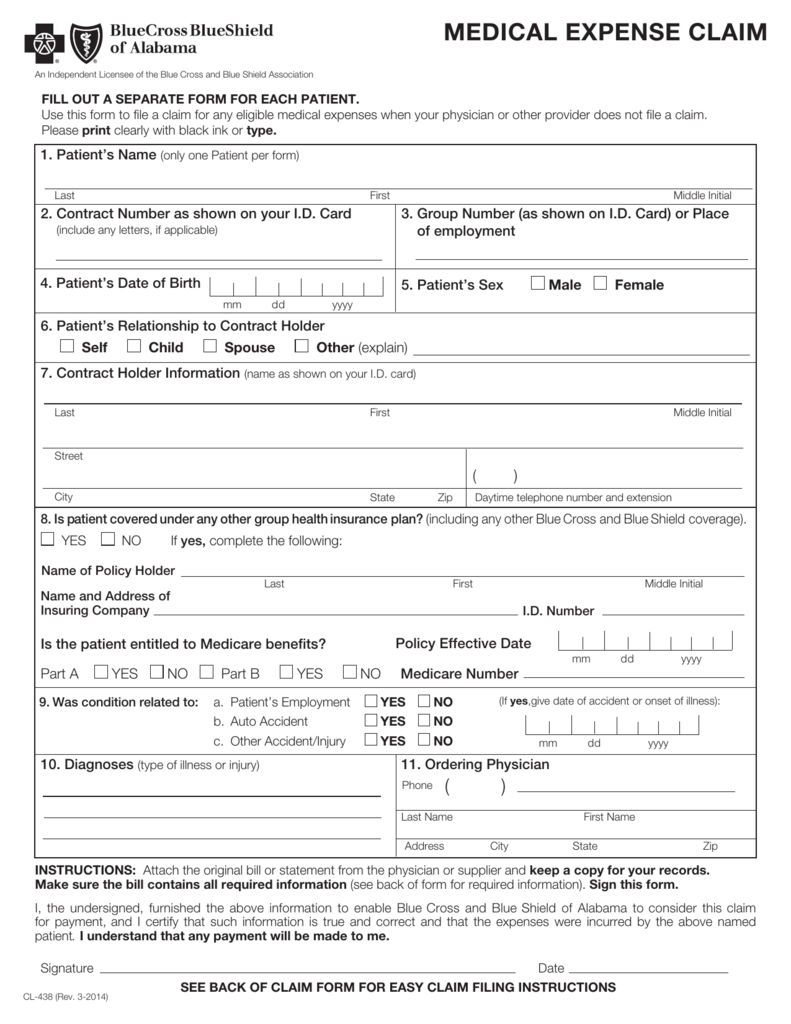 Cl 438 Medical Expense Claim Form
Cl 438 Medical Expense Claim Form
 Blue Cross Blue Shield International Medical Claim Form Pdf Format E Database Org
Blue Cross Blue Shield International Medical Claim Form Pdf Format E Database Org
Blue Cross Blue Shield International Medical Claim Form Pdfsimpli
 Free Blue Cross Blue Shield Association Member Claim Form Pdf 90kb 2 Page S Page 2
Free Blue Cross Blue Shield Association Member Claim Form Pdf 90kb 2 Page S Page 2
 24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
24 Printable Blue Cross Blue Shield Vision Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
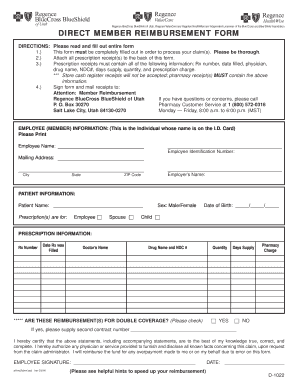 Regence Blue Shield Direct Member Reimbursement Form Fillable Fill Online Printable Fillable Blank Pdffiller
Regence Blue Shield Direct Member Reimbursement Form Fillable Fill Online Printable Fillable Blank Pdffiller
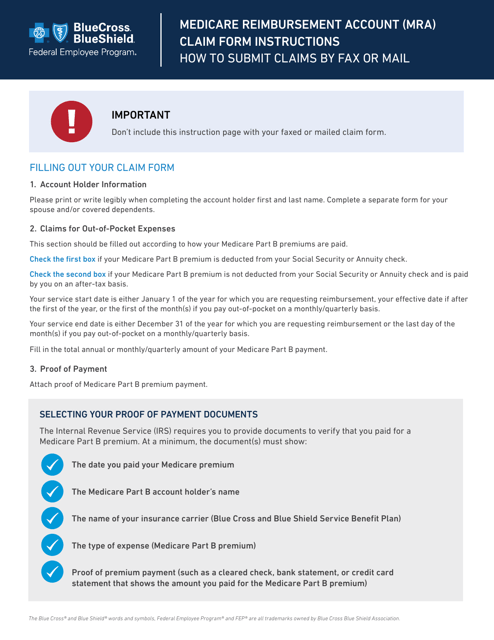 Form 4416 Bcbs Mra Pmb Frm Download Printable Pdf Or Fill Online Medicare Reimbursement Account Mra Claim Form Bluecross Blueshield Templateroller
Form 4416 Bcbs Mra Pmb Frm Download Printable Pdf Or Fill Online Medicare Reimbursement Account Mra Claim Form Bluecross Blueshield Templateroller
 Federal Bcbs Basic Overseas Claim Form Fill Out And Sign Printable Pdf Template Signnow
Federal Bcbs Basic Overseas Claim Form Fill Out And Sign Printable Pdf Template Signnow


Comments
Post a Comment