This form template authorizes your healthcare provider to release your private medical records to the parties you specify. Back to Forms By Program NOTE.
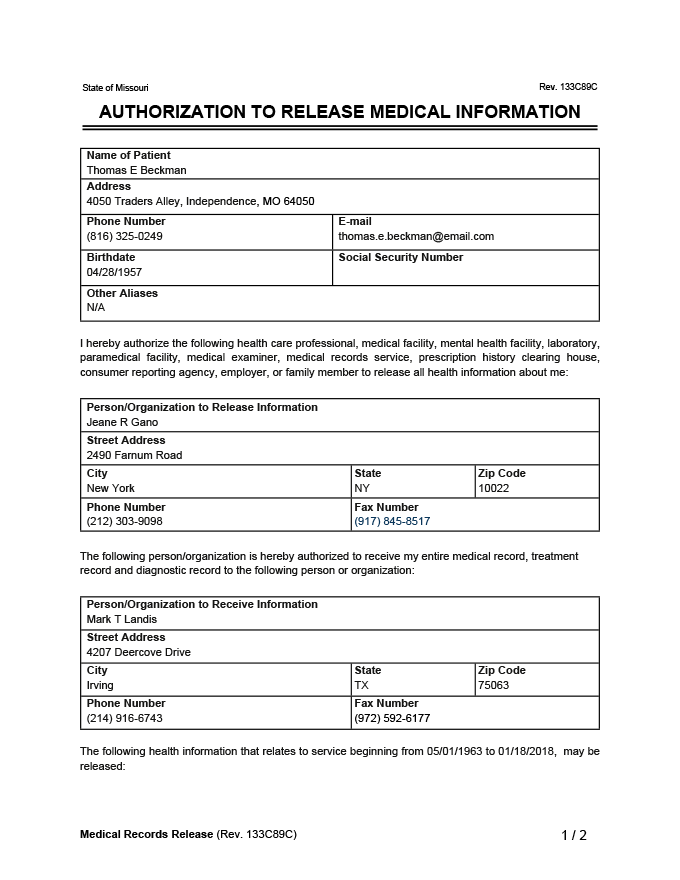 Medical Records Release Form Generic Request Template Pdf
Medical Records Release Form Generic Request Template Pdf
Medical Record Authorization Form Instructions.
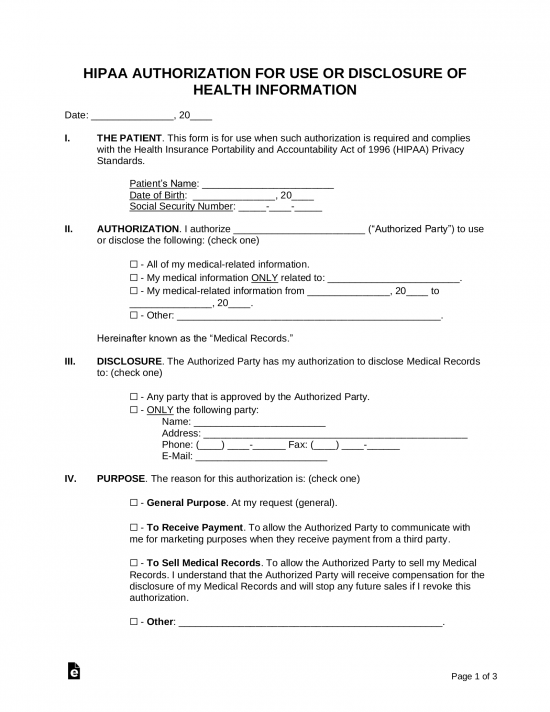
Medical release form california. Authorization to release healthcare information. Use this form to obtain the required authorization when a request is received for patient information unless the request received is a facsimile of this form or. _____ types in the PURPOSE section below q.
AUTHORIZATION FOR RELEASE OF PROTECTED HEALTH INFORMATION TO THIRD PARTIES DHCS 6247 File Number. Some links on this page are documents in Adobe Acrobat Portable Document Format PDF. STATE OF CALIFORNIA - HEALTH AND HUMAN SERVICES AGENCY CALIFORNIA DEPARTMENT OF SOCIAL SERVICES.
Completion of this document authorizes the disclosure and use of health information about. Physicians will require a patient to sign a records release form to transfer records. CW 61 701 AUTHORIZATION TO RELEASE MEDICAL INFORMATION Author.
Authorization for Release of Information to a third-Party a Non-UCLA Provider Insurance Company Attorney etc Authorization for Release of Health Information - English. Pages 3 4. If you need to install or upgrade to the latest version click the Download Free Readers.
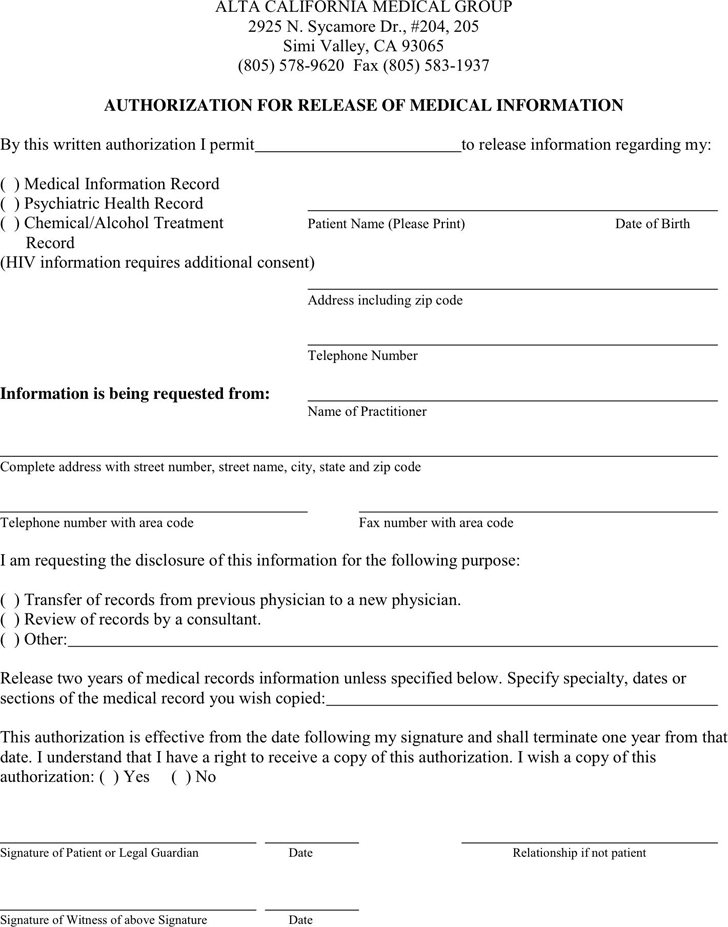
Physician clinic hospital hospice home health agency attending nurse psychologist counselor therapist etc i hereby authorize you to release any and all med. DEPARTMENT OF HEALTH CARE SERVICES PRIVACY OFFICE. Page 1 of 3.
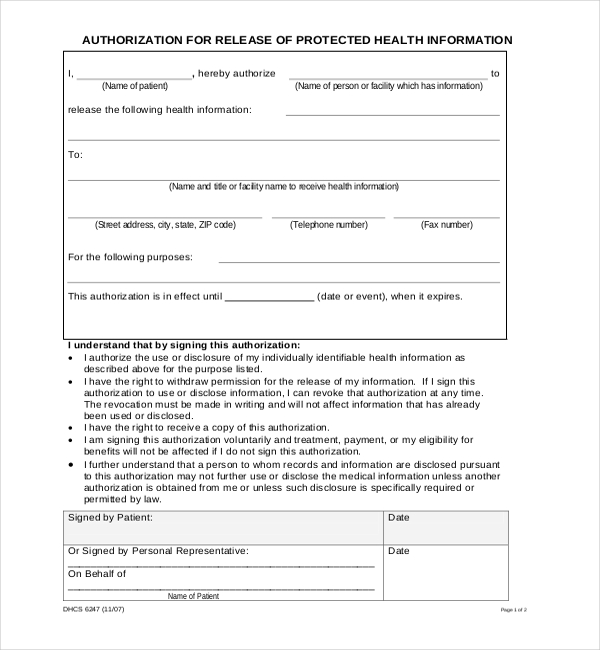
Please use Internet Explorer or download and open forms with Adobe Acrobat. The health information disclosed may only be used for the following purposes. AUTHORIZATION FOR RELEASE Confidential Patient Information.
State of california health and human services agency california department of social services community care licensing. Below are all forms used by the Medical Board of California. Complete and sign the form.
Page 1 of 2 Instructions. 1019 DEPARTMENT OF CORRECTIONS AND REHABILITATION Form. Release of clientresident medical information.
Must include a provision that allows release of medical records o or some other form of documentation. License Verification System LVS Licensees. STATE OF CALIFORNIA-HEALTH AND HUMAN SERVICES AGENCY.
DRIVER MEDICAL EVALUATION Medical information is CONFIDENTIAL under California Vehicle Code 18085 CVC INSTRUCTIONS TO THE DRIVER. I _____ authorize the release of health care information PRINT NAME related to my physical andor mental condition to the In-Home Supportive Services program as it pertains to my need for domesticrelated and personal care services. If you have followed the requirements outlined in the Health Safety Code and the physician has not complied with your request you may file a complaint with the Medical Board.
HIPAA Privacy Rule CFR Section 164508. I have read this form or had this form read to me. Download and print the Authorization for Release of Health Information form below.
STATE OF CALIFORNIA AUTHORIZATION FOR RELEASE OF PROTECTED HEALTH INFORMATION CDCR 7385 Rev. Failure to provide all information requested may invalidate this authorization. If you need assistance filling them out contact our Consumer Information Unit at 916 263-2382.
California Pacific Medical Center California Davies Pacific Van Ness Campuses San Francisco. Autorización para la Divulgación de Información Médica - Spanish. Unless indicated are smaller than 2 MB.
Judicial Council of California wwwcourtscagov JV-226 Page 1 of 3 Revised July 1 2013 Optional Form JV-226 Authorization to Release Health and Mental Health Information I am the This form authorizes the release of the childs health andor mental health records to. Use NA if not applicable. AUTHORIZATION FOR RELEASE OF PROTECTED HEALTH INFORMATION.
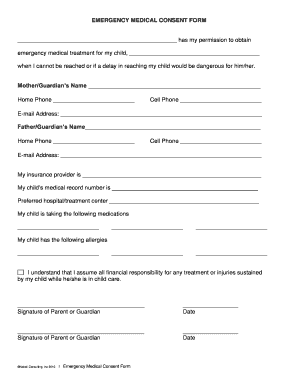
Release the following health information. AUTHORIZATION AND CONSENT AND RELEASE I hereby certify that my child is in good health and can travel to and participate in all functions of the 4-H Youth Development Program as described above. Five-level outline with instructions Word Sports.
California Hospital Association - Form Made Fillable by eForms. OF PATIENT INFORMATION See WI Code Section 5328 and. All sections must be completed for the authorization to be honored.
I am the parentguardian having legal custody of the youth member named above as stated under California Family Code Section 6550. PO Box 619091. Allow named KP physician to view records PURPOSE.
I Name of patient hereby authorize Name of person or facility which has information to. Complete forms Please specify form Telephone number. Fax or mail the completed form to.
USE AND DISCLOSURE OF HEALTH INFORMATION. Before giving this form to your medical professional complete and sign Sections 1-3. PDF documents require Adobe Reader.
FOR COPIES SPECIFY THE HEALTH INFORMATION NEEDED FOR USE OR DISCLOSURE. CA Dept of SOcial Services. More templates like this.
_____ By completing this form you are authorizing the California Department of Health Care Services to release your protected health information identified herein to the persons or entities identified herein. Please take this form to the medical professional most familiar with your health history and current medical condition.
 California Youth Medical Release Form Pdfsimpli
California Youth Medical Release Form Pdfsimpli
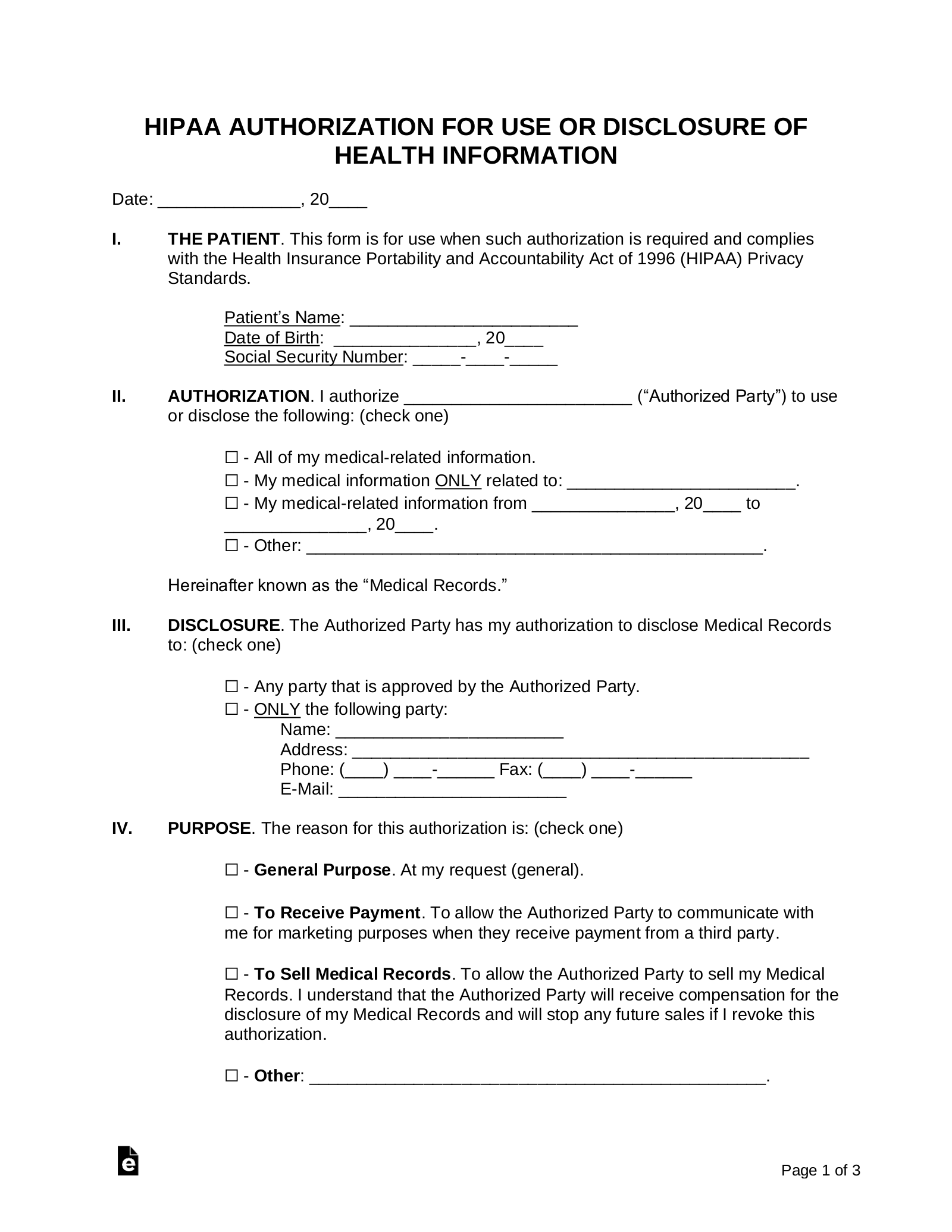 Free Medical Records Release Authorization Form Hipaa Word Pdf Eforms
Free Medical Records Release Authorization Form Hipaa Word Pdf Eforms
 Generic Medical Release Form Pdf Fill Out And Sign Printable Pdf Template Signnow
Generic Medical Release Form Pdf Fill Out And Sign Printable Pdf Template Signnow
 23 Printable Medical Release Form Templates Fillable Samples In Pdf Word To Download Pdffiller
23 Printable Medical Release Form Templates Fillable Samples In Pdf Word To Download Pdffiller
 Free Medical Records Release Authorization Form Hipaa Word Pdf Eforms
Free Medical Records Release Authorization Form Hipaa Word Pdf Eforms
 Free California Authorization For Release Of Medical Information Pdf 16kb 2 Page S
Free California Authorization For Release Of Medical Information Pdf 16kb 2 Page S
 Free 21 Sample Medical Records Release Forms In Pdf Word Excel
Free 21 Sample Medical Records Release Forms In Pdf Word Excel
 California Medical Release Form Pdfsimpli
California Medical Release Form Pdfsimpli
 Download California Medical Records Release Form For Free Formtemplate
Download California Medical Records Release Form For Free Formtemplate
 California Medical Release Form Pdf Format E Database Org
California Medical Release Form Pdf Format E Database Org
Bill Of Sale Form California Authorization For Release Of Medical Information Templates Fillable Printable Samples For Pdf Word Pdffiller
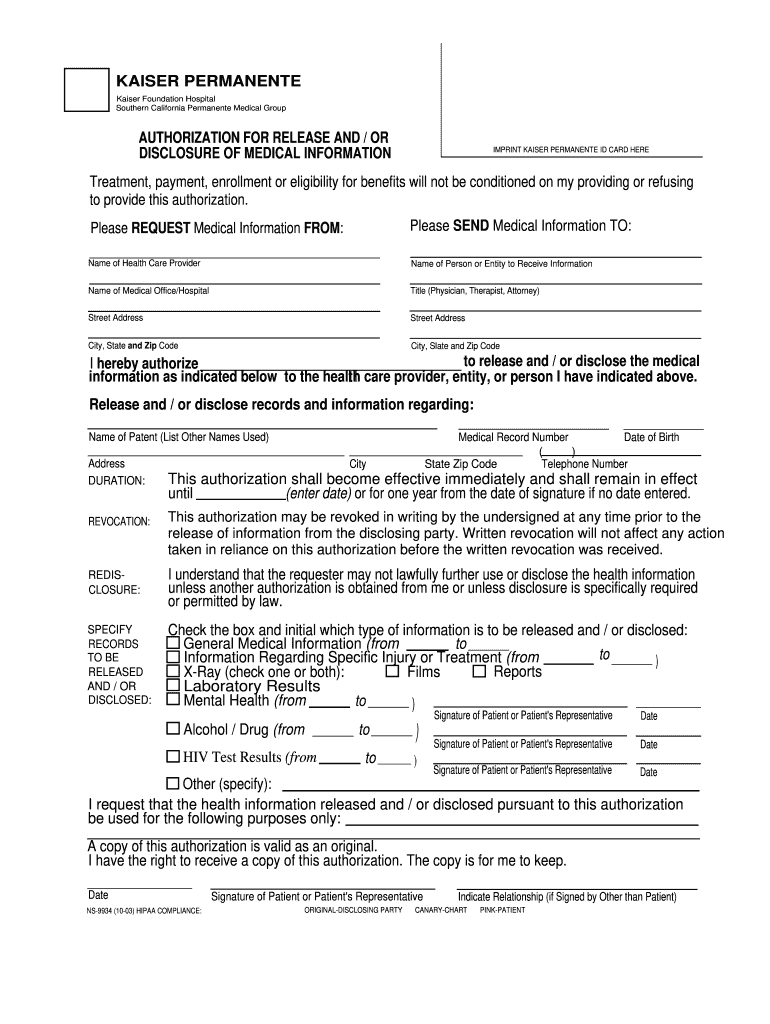 Kaiser Medical Records Release Form California Fill Online Printable Fillable Blank Pdffiller
Kaiser Medical Records Release Form California Fill Online Printable Fillable Blank Pdffiller
 Free 22 Sample Medical Release Forms In Pdf Word Excel
Free 22 Sample Medical Release Forms In Pdf Word Excel
 California Medical Release Form Download The Free Printable Basic Blank Medical Release Form Template Or Waiver I Medical Medical Technician Emergency Medical
California Medical Release Form Download The Free Printable Basic Blank Medical Release Form Template Or Waiver I Medical Medical Technician Emergency Medical


Comments
Post a Comment