BCBSILs policy requires that you the employee enroll in order to also enroll your dependents. Sole ProprietorOwnerOfficer Statement for those not listed on DE6.
 Https Www Blueshieldca Com Provider Content Assets Documents Miscpdfs Guidelinesresources Forms C14876 Fillin 3 13 Pdf
Https Www Blueshieldca Com Provider Content Assets Documents Miscpdfs Guidelinesresources Forms C14876 Fillin 3 13 Pdf
Download Blue Shield of California Small Group Application.
Blue shield of california application form. English Spanish Chinese Vietnamese. 10 Zeilen This form is for retirees who want to enroll in Blue Shield of California Medicare. During tax season Covered California sends two forms to our members.
To enroll in Blue Shield of California Medicare Rx Plan please provide the following Information. The federal IRS Form 1095-A Health Insurance Marketplace Statement and the California Form FTB 3895 California Health Insurance Marketplace Statement. Begin identifying individuals who qualify for the subsidy and their last known address.
Health plans are offered by Blue Shield of California. And mail it to the address below postmarked by _____ in order for your claim to be considered. Your signature and the date are required WAIVER OF COVERAGE.
C12914 421 Employee Application 1 of 9 Blue Shield of California is an in dependent member of the Blue Shield As so ciation C12914-FF 421 Small Business Employee Enrollment Form Blue Shield of California and Blue Shield of California Life. Individual Practitioner Information Change Form PDF 12 MB Individual Practitioner Record Application PDF 279 KB Physician Specialty Attestation PDF 90 KB. Please read date and sign this Section.
IM Applications PO Box 3008 Lodi CA 95241-9969 or fax. Covered by the blue shield of california. You must sign the claim form certification in.
Employee Application for each eligible employee owner or officer. Blue Shield may use any medical information in reviewing an individuals application including any medical condition that occurs after the signature and submission of the application and before an underwriting decision is made or before the effective date of coverage. Employer Notification of Qualifying Events under Cal-COBRA ENF Complete this form when covered employees have an event that qualifies them for coverage under the California Continuation Benefits Replacement Act Cal-COBRA California Senate Bill 719 Download.
Select the appropriate form to get started. If necessary use a separate piece of paper and attach it to this application. CoverMyMeds is Blue Shield of California Prior Authorization Formss Preferred Method for Receiving ePA Requests.
Blue Cross Blue Shield. Applications from all enrolling employees and dependents either paper Blue Shield Employee Enrollment spreadsheet or online portal Refusal of Coverage form s for all eligible employees and any eligible dependents who refuse or waive coverage at the time of open enrollment either paper Blue Shield Employee Enrollment spreadsheet or online portal. Pages 1 through 12 as your complete application including any other supporting documentation to Blue Shield Attn.
Download and submit Blue Shield forms that help you and your office meet credentialling requirements and other procedures. Download and review model notices and requirements from DOL published 472021. Youll need Adobe Reader to view the forms.
Apply to the blue shield of california authorization request form and certain amounts of forms for taking an approval before they are taking is one of coverage. Decide whether to adopt the alternative coverage election feature. Code Plan type Market code 1 Provide ALL requested information and print clearly in blue or black ink.
CoverMyMeds automates the prior authorization PA process making it the fastest and easiest way to review complete and track PA requests. Blue Shield of California is an HMO and PDP plan with a Medicare contract. Call Blue Shield at 800 431-2809 or contact your agent for help filling out the.
Application for Blue Shield of California Medicare Supplement plans FOR OFFICE USE ONLY Heres how to apply Accept. 2021 Enrollment Request Form Blue Shield of California Medicare Rx Plan PDP Employer GroupUnion Health Plan Please contact Blue Shield of California Medicare Rx Plan if you need information in another language or format Braille. The following documents can be emailed faxed or mailed to us.
Small Group Applications for Blue Shield of California. If you have a disability and need assistance applying for a position with Blue Shield of California call RehabWest Inc. 2 Sign and date in all places indicated.
Enrollment in Blue Shield of California. SIGNATURE LINE FOR NEWCHANGING COVERAGE. Update existing COBRA notices to include the required information.
Blue Shield of California uses Electronic Employment verification. Only a Blue Shield underwriter may make the final decision to accept.
 2018 2021 Form Ca Blue Shield A46163 Fill Online Printable Fillable Blank Pdffiller
2018 2021 Form Ca Blue Shield A46163 Fill Online Printable Fillable Blank Pdffiller
 Syscalls In Charge Toll Fill Online Printable Fillable Blank Pdffiller
Syscalls In Charge Toll Fill Online Printable Fillable Blank Pdffiller
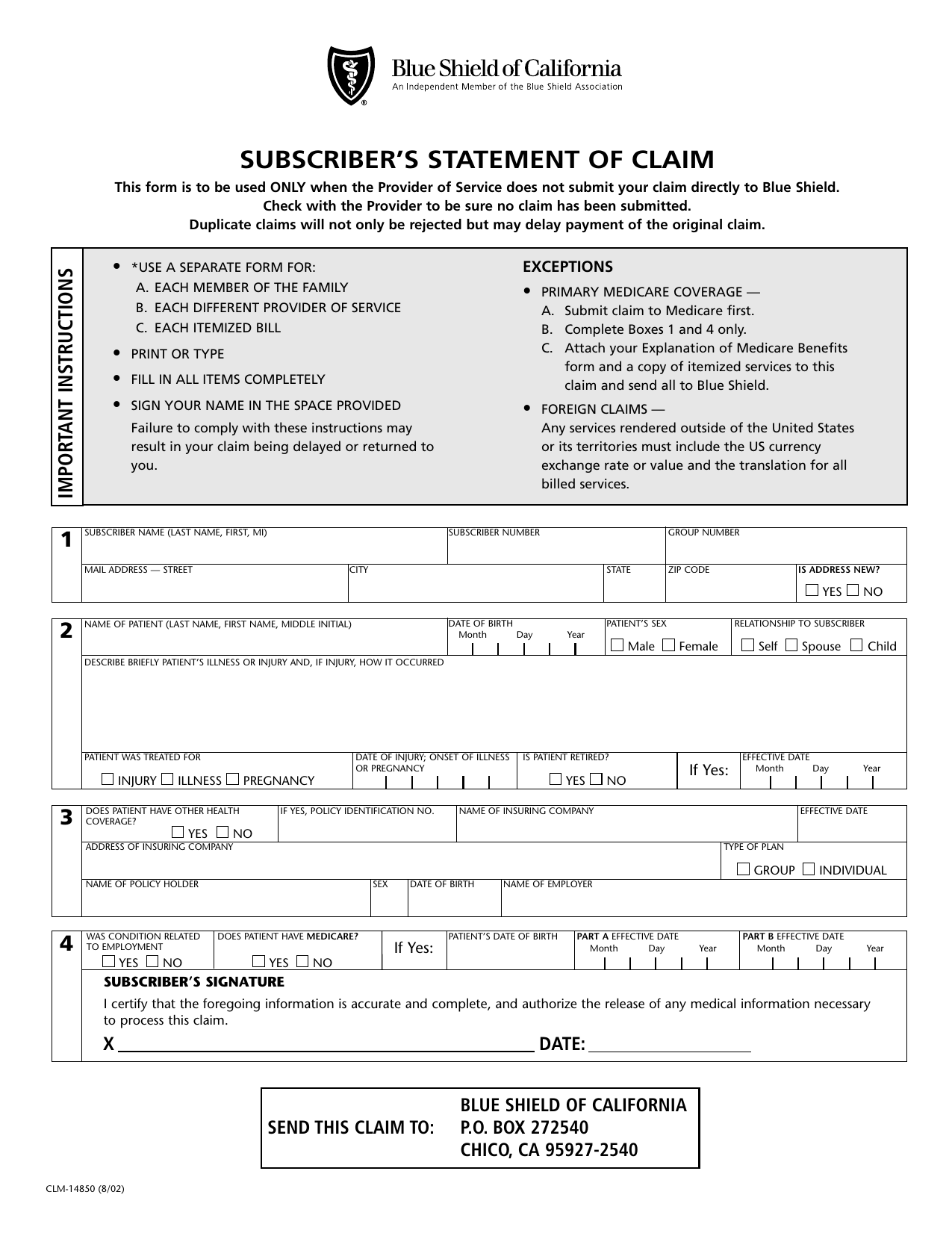
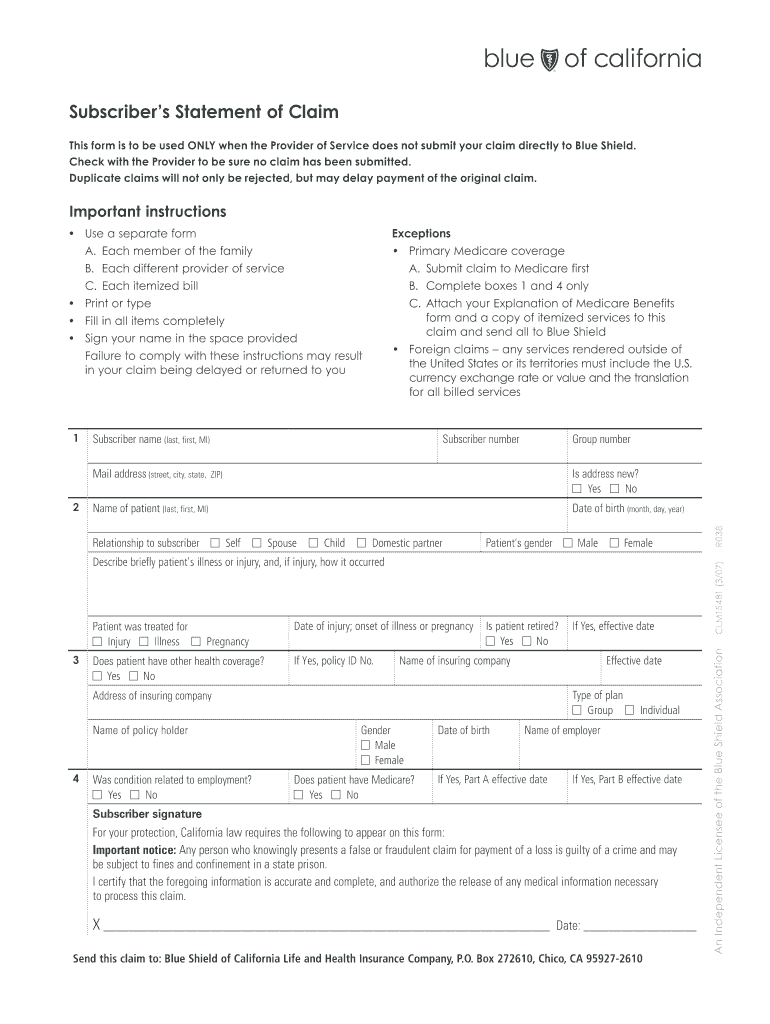 Blue Shield Of California Subscribers Statement Of Claim Form Fill Online Printable Fillable Blank Pdffiller
Blue Shield Of California Subscribers Statement Of Claim Form Fill Online Printable Fillable Blank Pdffiller
 Document 12087802
Document 12087802
 Https Files Covid19 Ca Gov Pdf Blue Shield Of California Govops Pdf
Https Files Covid19 Ca Gov Pdf Blue Shield Of California Govops Pdf
 Fillable Online Blue Shield Of California Individual Application Fillible Form Fax Email Print Pdffiller
Fillable Online Blue Shield Of California Individual Application Fillible Form Fax Email Print Pdffiller
 Blue Shield Of California Provides 300 000 To Support Youth Development Social Justice And Health Equity In Communities Of Color
Blue Shield Of California Provides 300 000 To Support Youth Development Social Justice And Health Equity In Communities Of Color
 Https Www Blueshieldca Com Sites Oc Documents Medical Claim Form 10 7 V1 Pdf
Https Www Blueshieldca Com Sites Oc Documents Medical Claim Form 10 7 V1 Pdf
 Https Www Blueshieldca Com Bsca Documents Find A Plan Health Plans Individual Family C12900 Rd Ext 1 13 Pdf
Https Www Blueshieldca Com Bsca Documents Find A Plan Health Plans Individual Family C12900 Rd Ext 1 13 Pdf
 Https Www Blueshieldca Com Bsca Bsc Public Broker Portalcomponents Streamdocumentservlet Filename C12687 Pr Pdf
Https Www Blueshieldca Com Bsca Bsc Public Broker Portalcomponents Streamdocumentservlet Filename C12687 Pr Pdf
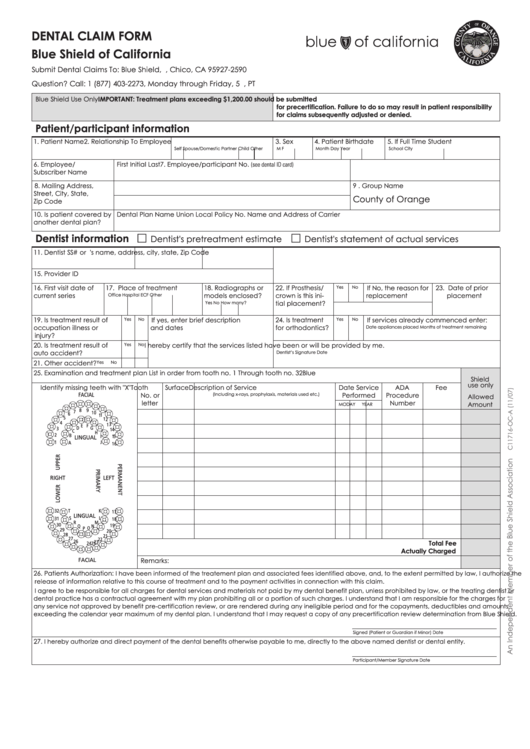
Dental Claim Form Blue Shield Of California Printable Pdf Download
 Forms And Applications Producer Connection
Forms And Applications Producer Connection
 21 Printable Blue Cross Blue Shield Health Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
21 Printable Blue Cross Blue Shield Health Reimbursement Form Templates Fillable Samples In Pdf Word To Download Pdffiller
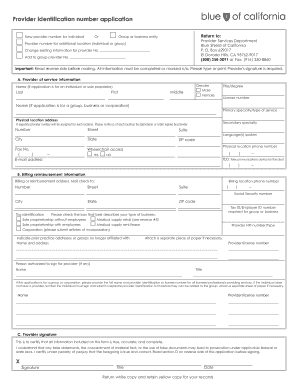 Fillable Online Blue Shield Of California Provider Identification Number Application Form Fax Email Print Pdffiller
Fillable Online Blue Shield Of California Provider Identification Number Application Form Fax Email Print Pdffiller


Comments
Post a Comment